I often forget that I have not had the pleasure of actually meeting most of you face-to-face before, and it is a challenge that I face when I assume that you all know what makes fuels my fire for knowledge as not only a clinical nutritionist, scientist, healthcare practitioner, but as a general human being.
I have many areas of health that I am passionate about, and as a clinical nutritionist I am (and have to be) across the board qualified to treat any and all cases that come through my door, whether that be for the cold you’ve come down with, someone with a complex autoimmune condition, someone who is desperate to lose weight for their upcoming wedding or a baby who is failing to thrive. And my #1 specialty is methylation & MTHFR genetic health.
Why is it that I know so much and choose to specialise in this MTHFR genetic mutation? Simply because I am personally affected by this condition myself (being C677T + A1298C compound heterozygous myself), and I want the best management and up to date science behind the dysfunctional genetic mutations, not just for myself but for all that pass through my clinic on a daily basis. I have spent literally thousands of hours doing further research and attending conferences to be the best practitioner I can be, for the health & wellbeing by identifying, managing and supporting my clients with their own MTHFR mutations. For the record, MTHFR is short for Methylenetetrahydrofolate Reductase, obviously a total mouthful, hence the abbreviation.
I often find myself being approached by those who have had conception struggles or [often multiple] miscarriages, mental health issues such as depression/anxiety, chronic fatigue, cardiovascular disease (heart attacks, strokes, etc), allergies, or even those who simply find they cannot lose any weight no matter what they do. And they all send off genetic alarm bells in my mind and I go through a mental checklist of health concerns that qualify for MTHFR genetic testing. And there is so much I can do to help, yet many simply don’t come and ask at the beginning of their health journey as they just don’t understand that all that they experience is connected to something greater and much deeper than the symptoms they experience.
If only I received $1 for every time I have heard a client say “Oh my goodness, if only I knew about you before now, I could have avoided XYZ from happening and I would be so much better/healthier/happier than I am today, if only I knew…“. Well, you know now!
When the MTHFR gene is functioning properly, it is highly efficient at helping our bodies convert vitamin B9 (folate) into a usable form called methylfolate. When this gene is mutated, this capacity to convert vitamin B9 into methylfolate is reduced by 40-70%. That is the whole issue here, because the conversion of folic acid into a useable form is absolutely essential for DNA synthesis and repair, neurotransmitter production, detoxification, and immune function.
**A quick word on Vitamin B9 – Folate. Folic acid is a synthetic/man-made version of B9, found in supplements and fortified foods, while folate occurs naturally in foods.**
Methylation itself begins with a methyl group, which is stuck together with a carbon and three hydrogen atoms. Methylation is responsible for countless critical functions within the body, such as:
- * Turns genes on and off,
- * Repairs and builds DNA & RNA,
- * Reduces the ageing process (protects telomeres),
- * Detoxifies chemicals & heavy metals,
- * Processes hormones,
- * Builds immune cells,
- * Turns the stress response on and off,
- * Provides us with energy,
- * Reduces histamine (prevents allergies),
- * Repairs cell membranes and produces myelination of nerves,
- * Supports neurotransmitters to prevent depression, anxiety, insomnia and help brain function.
The methylation process occurs within cycles, and this is where the MTHFR genetic mutation comes into it. MTHFR is a complex enzyme that adds a methyl group to folic acid to allow the human body to use it.
This MTHFR gene is responsible for the production of this enzyme that is necessary for properly using vitamin B9 (folic acid). This enzyme is also important for converting homocysteine into methionine (required by the body for proper metabolism & muscle growth) that is also required to then create glutathione. And for those who don’t know, glutathione is the Mother of all antioxidants within the human body.
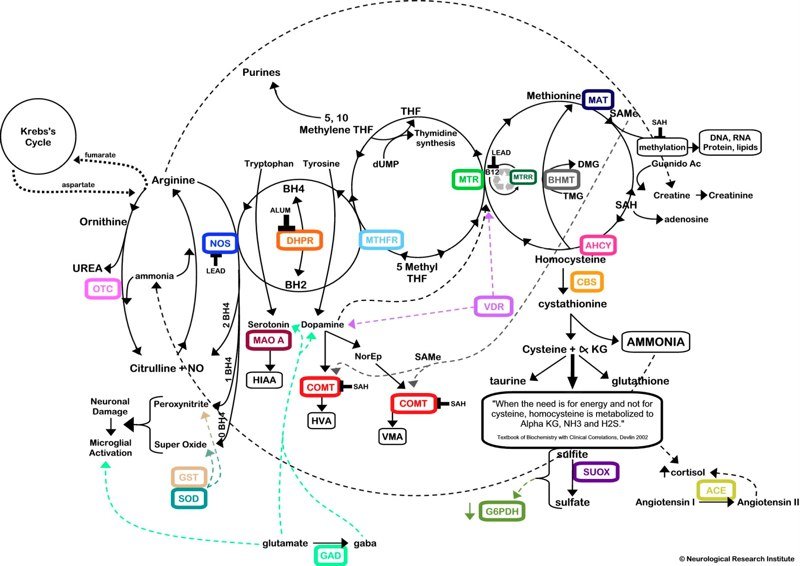
This process of methylation is extremely complex and involved many cycles (as seen in the image below), and includes the enzyme from the MTHFR gene, so anyone with a mutation may have trouble effectively eliminating toxins from the body.
In a nutshell, MTHFR variants are very common within the general population, meaning many will have it but not actually know it, and those that do know it is generally due to some kind of health concern that lead to a healthcare practitioner testing for it, but due to it not being very well understood by most GP’s it tends to fall by the wayside and remains untested.
In the past, many conditions such as strokes due to elevated homocysteine levels or women who experience a miscarriage, stillbirth, maternal thrombosis or baby born with cleft lip/palate, or born with a neural tube defect and other congenital cardiac abnormalities. These conditions are all closely linked to a positive MTHFR status.
MTHFR genetic mutations are passed on by the biological parents if both parents pass on a healthy gene, you won’t have any mutations at all. If one parent passes on a healthy gene, but the other passes on a mutated gene, several variations can occur. If both parents pass on a mutated form, there are many more scenarios that can occur.
There are other genetic dysmutations that can be passed on, however they are not often problematic. The C677T and A1298C genetic mutations cause the most health concerns.
The most common mutations within the MTHFR gene are:
- Heterozygous – having one copy of the C677T or A1298C mutation and one normal copy,
- Homozygous – having two copies of the C677T or A1298C mutation,
- Compound Heterozygous: where one parent passes on their C677T gene mutation and the other passes on their A1298C gene mutation.
The differences between C677T and A1298C
- Those with a C677T mutation are more likely to have elevated homocysteine, and may have a family history of cardiovascular disease such as stroke, heart attack, deep vein thrombosis,
- Those with an A1298C mutation are more likely have neurotransmitter disturbances/mental health issues such as inabilities to manage moods, emotions or stress levels, sensitivities to pain, concentration, and the ability to learn or even relax.
I am more than happy to write more on this issue if you wish, just comment below and tell me what you want to know more about and I’ll get writing.
If you think you may be affected by MTHFR or you would like a personalised consult with me, please head to my APPOINTMENTS PAGE to schedule in a consult with me, or an online Skype consult if you aren’t in Victoria, Australia.



0 Comments